
As National Addictions Awareness Week 2015 draws to a close, I want to explore the topic of harm reduction – an approach to drug strategy and policy that has become near and dear to me over the past several months, and one that organizations all over the globe are asking others to commit to.
Since starting my practicum at a community health centre, I’m often asked about what I do by my family and peers. Much of what I do is rooted in harm reduction: an area that is difficult for many people to understand. I get it, it does seem odd to outsiders why I would be spending my time handing out fresh pipes, screens, syringes and more to marginalized folks using drugs. Frequently, I’m asked if I think what I’m doing “enables” people to use drugs – insinuating that harm reduction increases drug use or makes it “worse” – and just perpetuates the issue. I find these kinds of questions come from a perspective in which all drug use is labeled “bad” and in which it is my job to ensure someone stops using – and this simply isn’t what harm reduction is about.
What is harm reduction?
As written in our Youth Employment Toolkit: “Harm reduction is often viewed negatively because of its link to substance use, but harm reduction approaches are used on a daily basis by the general population: hand washing, seat belts in cars, crosswalks and bike helmets.” So you can think of it as an approach that acknowledges that people do and will use drugs, and so instead focuses on limiting potential consequences.
Much like wearing a seatbelt doesn’t stop people from driving, harm reduction alone does not aim to reduce or stop drug use (though it often acts as a point of connection for people when they do decide that they want to use less). Most harm reduction services focus on providing clean and new supplies through needle distribution and exchange, supervised injection sites, street outreach, workshops, and even alcohol management programs. And it works. As Hedrich and Hartnoll wrote in their review of harm reduction interventions:
…the scientific evidence shows that harm reduction interventions are effective in terms of their stated goals, as long as they are implemented appropriately within their contextual settings; and…single interventions are far more effective when implemented together as part of a broader public health policy, including steps to facilitate healthier living and safer social environments.
Part of the bad rap harm reduction gets is this idea that it alone can address the complex issue of problematic drug use (and the often traumatic and systemic events that contribute to why some people use), which it just can’t. Harm reduction is about meeting the person where they’re at and encouraging them to change risky behaviour, not demanding that they stop using altogether.
BC Harm Reduction Strategies and Services outlines the following guiding principles for harm reduction: pragmatism (accepting that drug use has always and will likely always occur); human rights (basic dignity and respect for all); focus on harms (instead of the drug use); maximize intervention options (needing a variety of approaches); priority of immediate goals (what does the person need right now?); and drug user involvement (nothing for us without us). These principles are very important. People who use drugs are deeply stigmatized, and though not everyone who experiences homelessness uses drugs, it is a reality for many. The potential harms associated with substance use, as noted in our section on substance use, are many:
This includes pharmacological effects of the substance itself that may impair a person’s ability to safely and competently make decisions and carry out tasks that they engage in. Problematic substance use may lead to deteriorating health; accidental death; and increased chances of risky sexual behaviours. Other harms that may result from problematic use of substances include: the inability to work or stay in school, ruptured relations with family, friends and community members, and problems with the law.
I’d like to draw some attention to the last part about legal and justice issues. The criminalization of some substances – which is unrelated to potential harm caused, if we consider the great many negative effects associated with alcohol – means that many drug users themselves are also criminalized. This punitive, no-tolerance policy on some drugs has been criticized by many, including the writers of a 2014 London School of Economics report, which asks decision-makers to finally “end the drug wars.” The Canadian Drug Policy Coalition is making similar calls for action and advocates for policy “based on evidence, human rights, social inclusion and public health.” Harm reduction is a core component of such policy, largely due to a growing evidence base of its effectiveness.
Harm reduction in Canada
One primary goal of harm reduction is to reduce the contraction of blood-borne diseases among users. A 2010 international study by Wodak and Maher concluded that “countries that have provided extensive needle and syringe programs and opioid substitution treatment appear to have averted an epidemic, stabilised or substantially reduced the prevalence of HIV among injecting drug users.” As Vineeth wrote in his infographic post on World Hepatitis Day, harm reduction approaches have also seen great success in limiting the spread of hepatitis.
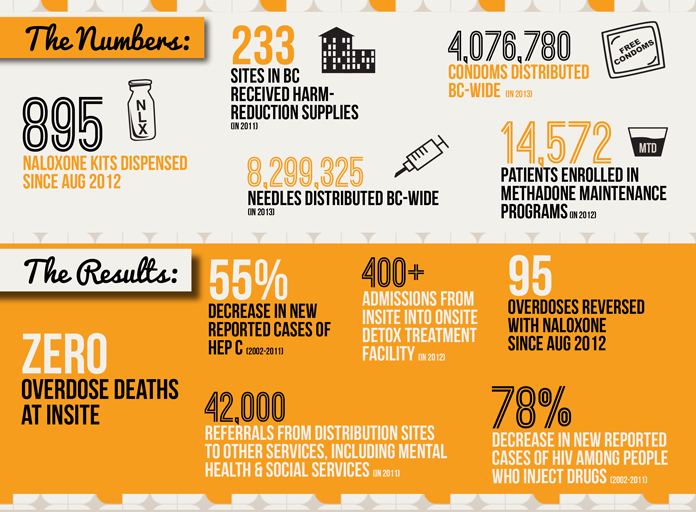
In Canada, British Columbia is a leader in coordinated harm reduction services (though Toronto is also considered a hub, with harm reduction as a key part of the city’s drug strategy) and in creating promising practices. The province has two supervised injection sites, implemented the first-ever crack pipe vending machine, and developed an alcohol management program. The Insite program has contributed to many positive results reported between 2002 and 2011:
- 0 fatal overdoses at Insite (since this post was initially written, there has been one)
- 78% decrease in new reported cases of HIV among people who inject drugs in the area
- 55% decrease in new reported cases of hepatitis C
Furthermore since 2012:
- 95 overdoses in the area have been reversed with naloxone
- 42,000 referrals made from distribution sites to other services (housing, mental health, etc.)
- 400+ admissions from Insite into onsite detox program
So while harm reduction doesn’t put a stop to problematic drug use – and no one strategy will – it certainly does save lives, reduce disease transmission, encourage coordination of services, and more. For those reasons alone, I’d say it’s more than an appropriate response.
For more information, check out: